
Brainstem hub for stopping pain signals from reaching the brain
Acute or short-lived pain, despite its bad reputation, is usually a lifesaver. It acts as a transient negative sensory experience that helps us avoid danger. Touch a hot stove, stub a toe, or bonk your head on a low branch, and the nervous system cues up an “Ow!” Over time, the sting fades, the wound heals, but the lesson sticks.
Chronic pain is different; the alarm keeps blaring long after the fire is out, and then the pain itself becomes the problem. Nearly 50 million people in the United States live with chronic pain, an invisible and often untreatable condition that can linger for decades. “It’s not just an injury that won’t heal,” says a neuroscientist, “it’s a brain input that’s become sensitized and hyperactive, and determining how to quiet that input could lead to better treatments.”
Now, research has identified a key to regulating long-term pain states: a group of cells called Y1 receptor (Y1R)-expressing neurons in the brainstem’s lateral parabrachial nucleus (lPBN). These neurons are activated during enduring pain states, but they also integrate information about hunger, fear and thirst, allowing for pain signals to be modulated by other brain circuits signaling more urgent needs.
Their findings, published in Nature, suggest that there is hope because “there are circuits in the brain that can reduce the activity of neurons that transmit the signal of pain.”
The researchers used calcium imaging to watch neurons fire in real time in preclinical models of acute and chronic pain. They found that Y1R neurons didn’t just flare briefly in response to acute pain—they also kept firing steadily during enduring pain, a state neuroscientists call “tonic activity.”
The authors liken this to an engine left idling, where signals of pain continued to rumble and tick even when outward signs of pain had faded. This persistent activity may encode the lasting pain state people feel long after an accident or surgery.
The drive to look deeper into these neurons grew out of a simple observation the team made—hunger could dampen long-term pain responses.
“From my own experience, I felt that when you’re really hungry you’ll do almost anything to get food,” the author says. “When it came to chronic, lingering pain, hunger seemed to be more powerful than Advil at reducing pain.”
They previously found that other urgent survival needs such as thirst and fear can also reduce enduring pain. That finding supported behavioral models, suggest filtering of sensory input at the parabrachial nucleus can block out long-lasting pain when other more acute needs exist.
“That told us the brain must have a built-in way of prioritizing urgent survival needs over pain, and we wanted to find the neurons responsible for that switch,” says the author.
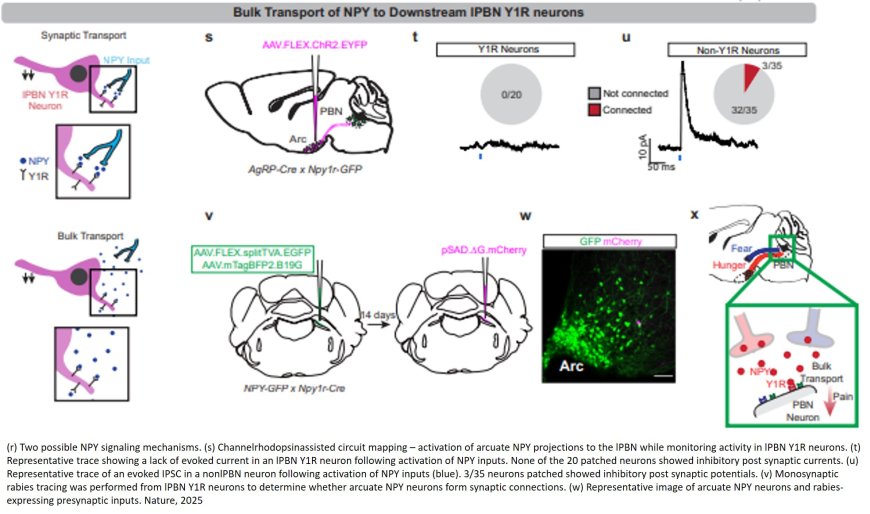
A key part of that switch is neuropeptide Y (NPY), a signaling molecule that helps the brain juggle competing needs. When hunger or fear takes priority, NPY acts on Y1 receptors in the parabrachial nucleus to dampen ongoing pain signals.
“It’s like the brain has this built-in override switch,” the author explains. “If you’re starving or facing a predator, you can’t afford to be overwhelmed by lingering pain. Neurons activated by these other threats release NPY, and NPY quiets the pain signal so that other survival needs take precedence.”
The researchers also characterized the molecular and anatomical identity of the Y1R neurons in the lPBN. They found that Y1Rneurons didn’t form two tidy anatomical or molecular populations. Instead, these neurons were scattered across many other cell types.
“It’s like looking at cars in a parking lot,” the author says. “We expected all the Y1R neurons to be a cluster of yellow cars parked together, but here the Y1R neurons are like yellow paint distributed across red cars, blue cars, and green cars. We don’t know exactly why, but we think this mosaic distribution may allow the brain to dampen different kinds of painful inputs across multiple circuits.”
This research also suggests that behavioral interventions such as exercise, meditation, and cognitive behavioral therapy may influence how these brain circuits fire, just as hunger and fear did in the lab.
“We’ve shown that this circuit is flexible, it can be dialed up or down,” the author says. “So, the future isn’t just about designing a pill. It’s also about asking how behavior, training, and lifestyle can change the way these neurons encode pain.”